Pass Your NCLEX® Exam on the First Try!
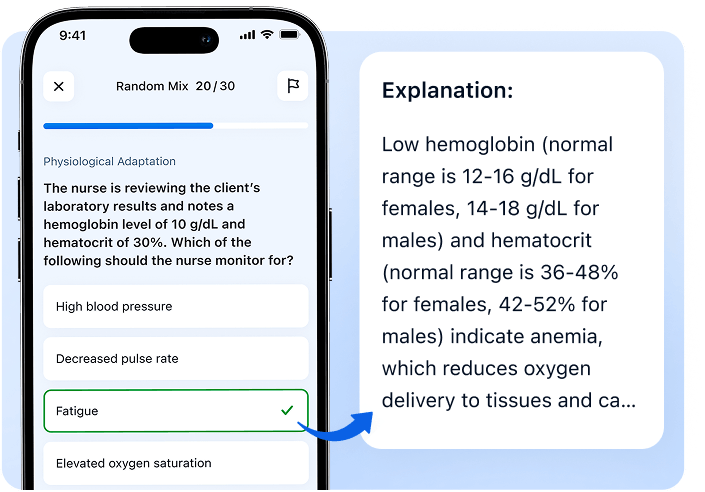
Try real NCLEX questions with explanations and unlock your personal study plan


Try real NCLEX questions with explanations and unlock your personal study plan
Answer several questions and get a personalized study plan built by expert nursing educators
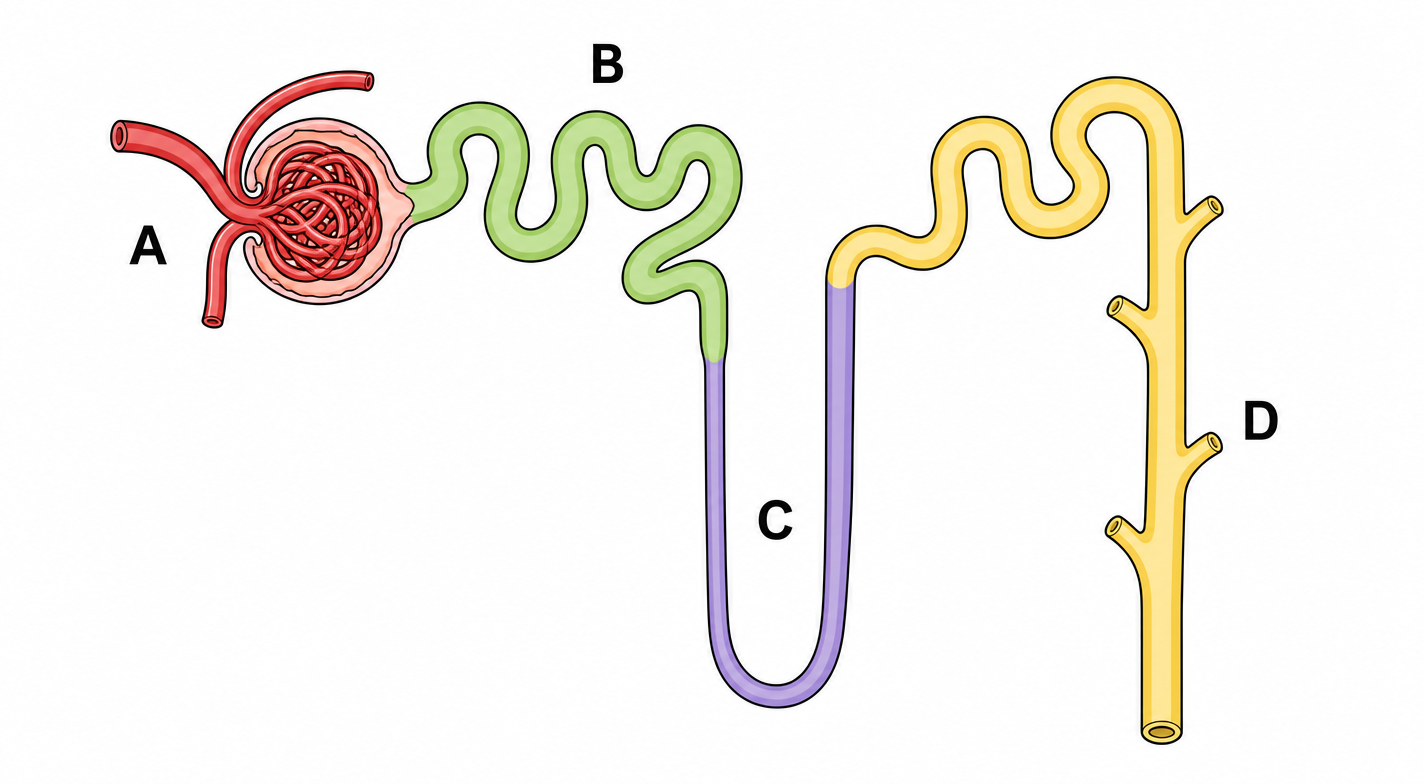
Segment D represents the distal convoluted tubule and collecting duct. Acute hypovolemia triggers ADH release from the posterior pituitary. ADH binds V2 receptors on the collecting duct → aquaporin-2 insertion → maximal water reabsorption. This is the direct mechanism behind oliguria and represents the fastest hormonal compensatory response to volume loss.
Segment A is the glomerulus, the site of filtration, not reabsorption. Glomerular pathology affects filtration rate (GFR), not the hormonal response to volume depletion seen here.
Segment B is the proximal convoluted tubule, which reabsorbs ~67% of filtered sodium and water constitutively. This is not hormonally upregulated in acute hypovolemia and does not represent the targeted compensatory mechanism here.
Segment C is the Loop of Henle, which establishes the medullary osmotic gradient essential for concentration. It is not a site of ADH action and plays no active role in the immediate hormonal compensatory response.
Segment D represents the distal convoluted tubule and collecting duct. Acute hypovolemia triggers ADH release from the posterior pituitary. ADH binds V2 receptors on the collecting duct → aquaporin-2 insertion → maximal water reabsorption. This is the direct mechanism behind oliguria and represents the fastest hormonal compensatory response to volume loss.
Segment A is the glomerulus, the site of filtration, not reabsorption. Glomerular pathology affects filtration rate (GFR), not the hormonal response to volume depletion seen here.
Segment B is the proximal convoluted tubule, which reabsorbs ~67% of filtered sodium and water constitutively. This is not hormonally upregulated in acute hypovolemia and does not represent the targeted compensatory mechanism here.
Segment C is the Loop of Henle, which establishes the medullary osmotic gradient essential for concentration. It is not a site of ADH action and plays no active role in the immediate hormonal compensatory response.
Hydrochlorothiazide causes sodium and water loss → compensatory proximal tubule reabsorption increases → lithium (handled similarly to sodium) is reabsorbed alongside → lithium clearance drops significantly → toxicity. HCTZ is the primary culprit here, compounded by already-reduced renal clearance evidenced by elevated creatinine.
Ibuprofen reduces renal prostaglandin synthesis → decreased GFR → reduced lithium clearance. This is a real and dangerous interaction, but the degree of lithium retention caused by thiazides is greater and more predictable. Contributing factor, not the primary one.
Attributing equal responsibility to both drugs misrepresents the pharmacokinetics. Thiazides carry the stronger and more direct interaction with lithium, this distinction matters for priority nursing action.
Lithium has a narrow therapeutic index (0.6–1.2 mEq/L), but toxicity at 2.8 mEq/L here is drug-interaction driven, not inevitable at standard dosing. Framing it as inherently toxic ignores the reversible, preventable cause.
Hydrochlorothiazide causes sodium and water loss → compensatory proximal tubule reabsorption increases → lithium (handled similarly to sodium) is reabsorbed alongside → lithium clearance drops significantly → toxicity. HCTZ is the primary culprit here, compounded by already-reduced renal clearance evidenced by elevated creatinine.
Ibuprofen reduces renal prostaglandin synthesis → decreased GFR → reduced lithium clearance. This is a real and dangerous interaction, but the degree of lithium retention caused by thiazides is greater and more predictable. Contributing factor, not the primary one.
Attributing equal responsibility to both drugs misrepresents the pharmacokinetics. Thiazides carry the stronger and more direct interaction with lithium, this distinction matters for priority nursing action.
Lithium has a narrow therapeutic index (0.6–1.2 mEq/L), but toxicity at 2.8 mEq/L here is drug-interaction driven, not inevitable at standard dosing. Framing it as inherently toxic ignores the reversible, preventable cause.
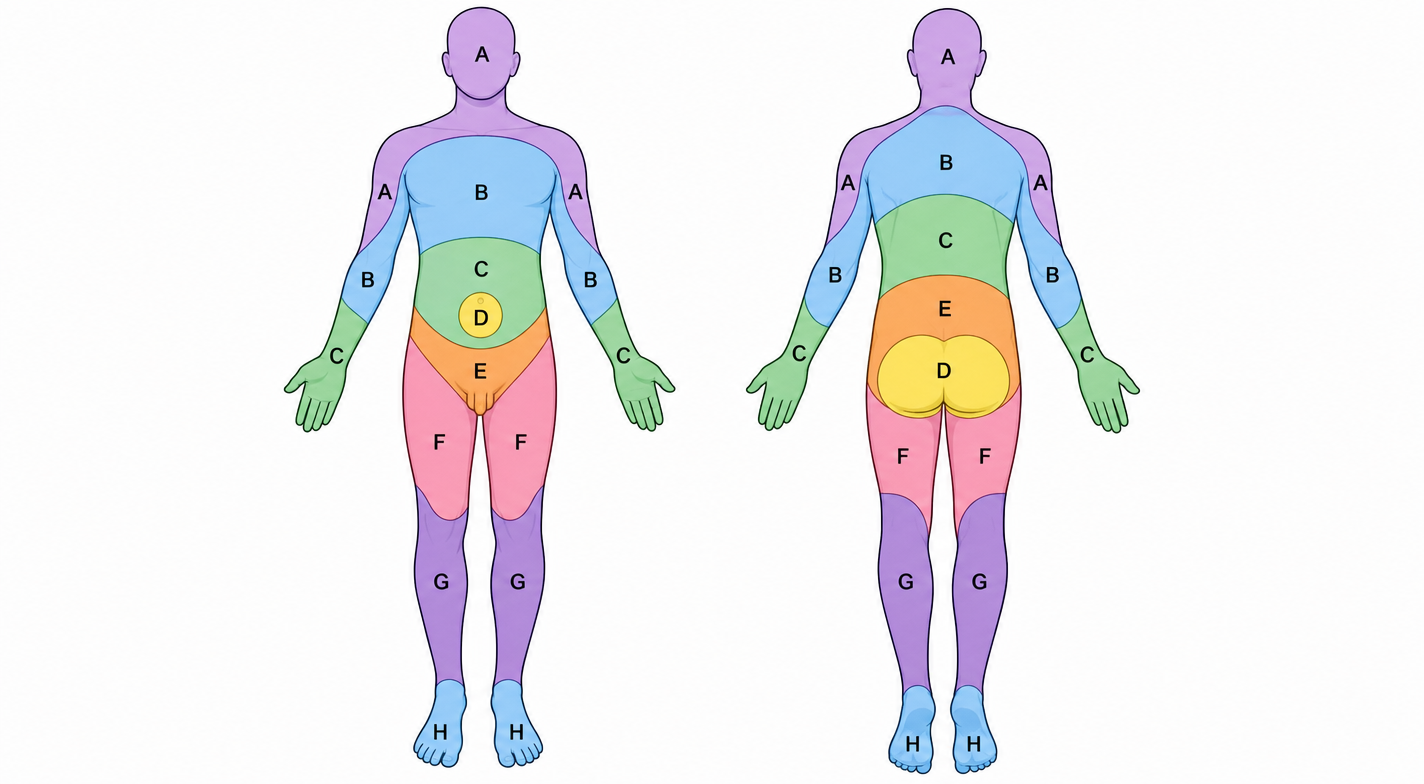
The umbilicus corresponds to the T10 dermatome, a high-yield anatomical landmark shown on the diagram. Loss of pain and temperature sensation with preserved proprioception suggests damage to the spinothalamic tract while the dorsal columns remain intact. This pattern supports a lesion around the T10 spinal level.
T6 corresponds to the upper abdomen near the xiphoid process. A lesion at this level would affect sensation higher on the torso and would not match sensory loss beginning below the umbilicus.
L1 corresponds to the inguinal region. A lesion here would spare the umbilical area and cannot explain the described sensory findings.
L4 affects the knee and medial leg. A lesion at this level is too distal to cause abdominal sensory loss around the umbilicus.
The umbilicus corresponds to the T10 dermatome, a high-yield anatomical landmark shown on the diagram. Loss of pain and temperature sensation with preserved proprioception suggests damage to the spinothalamic tract while the dorsal columns remain intact. This pattern supports a lesion around the T10 spinal level.
T6 corresponds to the upper abdomen near the xiphoid process. A lesion at this level would affect sensation higher on the torso and would not match sensory loss beginning below the umbilicus.
L1 corresponds to the inguinal region. A lesion here would spare the umbilical area and cannot explain the described sensory findings.
L4 affects the knee and medial leg. A lesion at this level is too distal to cause abdominal sensory loss around the umbilicus.
Sodium rose 14 mEq/L in 8 hours, safe correction limit is ≤10–12 mEq/L per 24 hours. Exceeding this rate causes osmotic demyelination syndrome (ODS): brain cells rapidly lose water following the osmotic shift, destroying myelin sheaths. New neurological symptoms after sodium correction are the classic warning sign and constitute a medical emergency.
Hyponatremia resolving as expected would present with clinical improvement, not new neurological deterioration. Rising sodium is correct in direction, but the rate is dangerous. Improvement and overcorrection are not mutually exclusive; new neuro symptoms shift the priority.
Hypernatremia requires sodium >145 mEq/L. At 132 mEq/L the patient remains hyponatremic, the danger here is the speed of correction, not the absolute value reached.
SIADH exacerbation would cause sodium to fall further, not rise. Rising sodium confirms the treatment is mechanically working, the problem is the rate, not treatment failure.
Sodium rose 14 mEq/L in 8 hours, safe correction limit is ≤10–12 mEq/L per 24 hours. Exceeding this rate causes osmotic demyelination syndrome (ODS): brain cells rapidly lose water following the osmotic shift, destroying myelin sheaths. New neurological symptoms after sodium correction are the classic warning sign and constitute a medical emergency.
Hyponatremia resolving as expected would present with clinical improvement, not new neurological deterioration. Rising sodium is correct in direction, but the rate is dangerous. Improvement and overcorrection are not mutually exclusive; new neuro symptoms shift the priority.
Hypernatremia requires sodium >145 mEq/L. At 132 mEq/L the patient remains hyponatremic, the danger here is the speed of correction, not the absolute value reached.
SIADH exacerbation would cause sodium to fall further, not rise. Rising sodium confirms the treatment is mechanically working, the problem is the rate, not treatment failure.
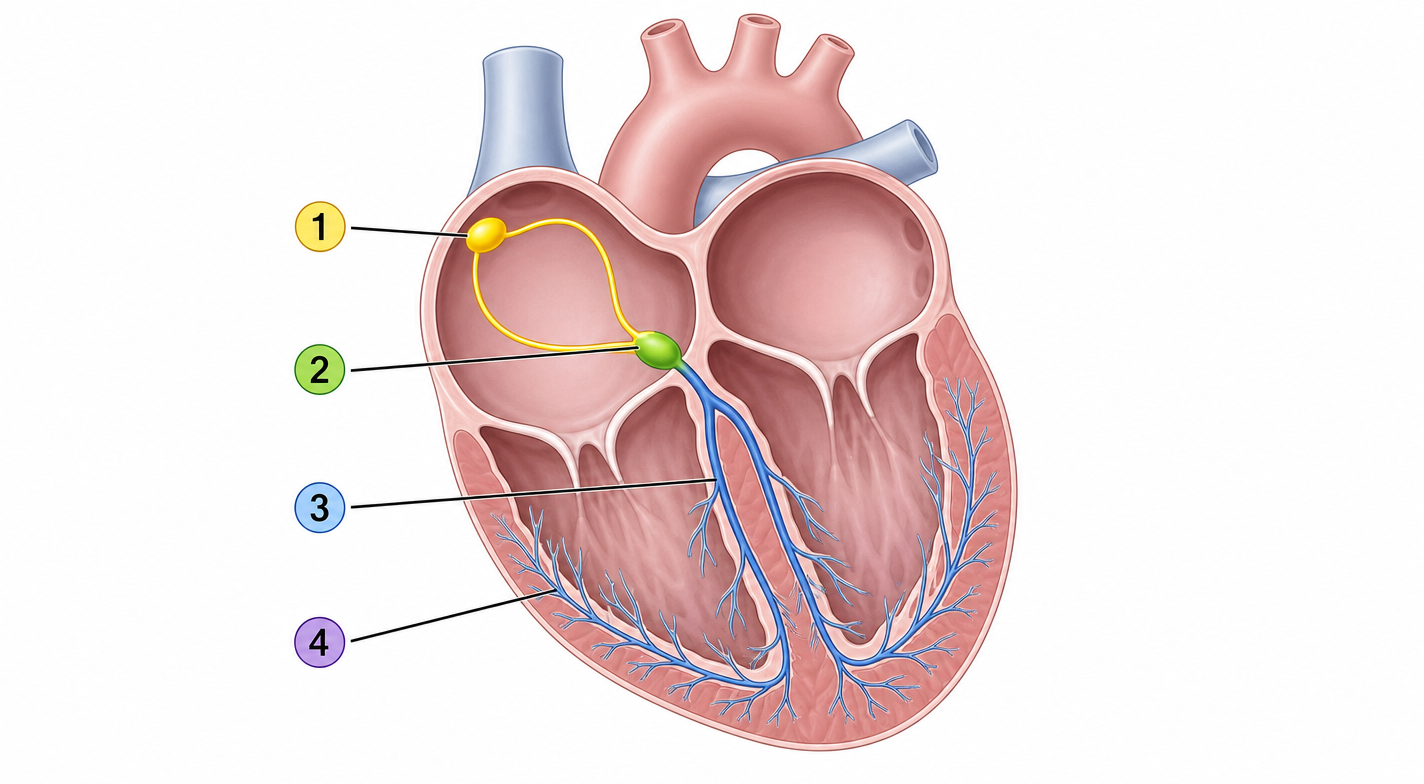
A prolonged PR interval with all P waves conducted describes first-degree AV block. The PR interval reflects conduction time from the SA node through the AV node, the delay occurs at Point 2 (AV node). No beats are dropped, distinguishing this from second or third-degree block. First-degree AV block is benign but requires monitoring for progression.
Point 1 is the SA node, the origin of the impulse. Pathology here affects rate and rhythm initiation (sick sinus syndrome), not PR prolongation. SA node dysfunction does not delay AV conduction.
Point 3 represents the Bundle of His and bundle branches. Delays here produce wide QRS complexes (bundle branch block), not PR prolongation. The QRS in this client is normal, ruling out infranodal delay.
Point 4 represents the Purkinje fibers. Conduction abnormalities at this level cause ventricular conduction defects and wide QRS, not a prolonged PR interval with narrow QRS as described here.
A prolonged PR interval with all P waves conducted describes first-degree AV block. The PR interval reflects conduction time from the SA node through the AV node, the delay occurs at Point 2 (AV node). No beats are dropped, distinguishing this from second or third-degree block. First-degree AV block is benign but requires monitoring for progression.
Point 1 is the SA node, the origin of the impulse. Pathology here affects rate and rhythm initiation (sick sinus syndrome), not PR prolongation. SA node dysfunction does not delay AV conduction.
Point 3 represents the Bundle of His and bundle branches. Delays here produce wide QRS complexes (bundle branch block), not PR prolongation. The QRS in this client is normal, ruling out infranodal delay.
Point 4 represents the Purkinje fibers. Conduction abnormalities at this level cause ventricular conduction defects and wide QRS, not a prolonged PR interval with narrow QRS as described here.
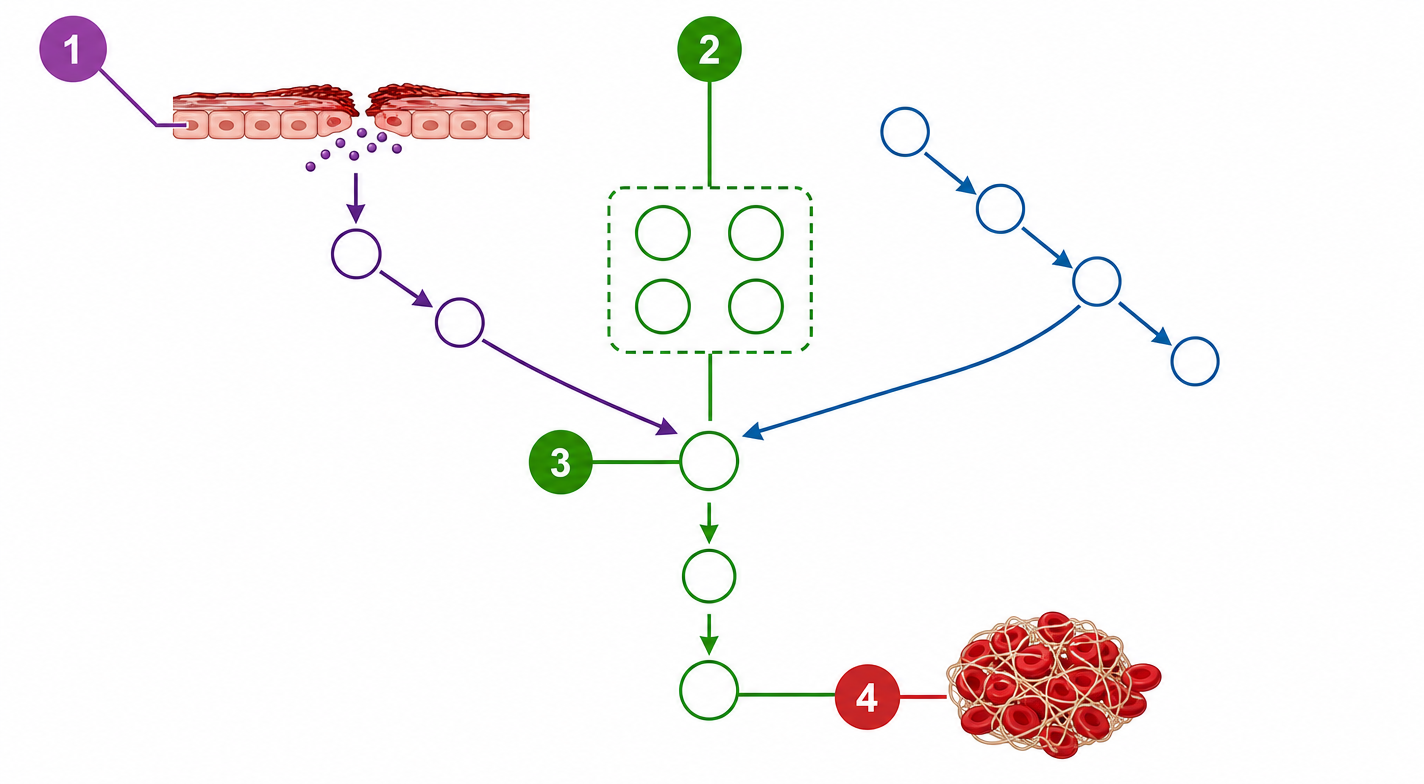
Heparin binds antithrombin III, dramatically enhancing its ability to inhibit thrombin and factor Xa, both acting at the common pathway represented by Point 3. aPTT of 140 seconds (therapeutic range 60–100 seconds) indicates supratherapeutic anticoagulation. Hematuria is a sign of bleeding complication. The LPN's priority is to report findings immediately to the supervising nurse or provider, reversal with protamine sulfate may be indicated.
Point 1 represents vascular injury and initiation of the cascade. Heparin does not act at this stage, it does not prevent vessel damage or initial platelet activation.
Point 2 represents activation of clotting factors via extrinsic and intrinsic pathways. Heparin's mechanism is downstream at the common pathway, not at the level of factor activation via tissue factor or contact activation.
Point 4 represents fibrin clot formation. Direct thrombin inhibitors such as argatroban act closer to this point. Heparin acts upstream by inhibiting thrombin before it can convert fibrinogen to fibrin.
Heparin binds antithrombin III, dramatically enhancing its ability to inhibit thrombin and factor Xa, both acting at the common pathway represented by Point 3. aPTT of 140 seconds (therapeutic range 60–100 seconds) indicates supratherapeutic anticoagulation. Hematuria is a sign of bleeding complication. The LPN's priority is to report findings immediately to the supervising nurse or provider, reversal with protamine sulfate may be indicated.
Point 1 represents vascular injury and initiation of the cascade. Heparin does not act at this stage, it does not prevent vessel damage or initial platelet activation.
Point 2 represents activation of clotting factors via extrinsic and intrinsic pathways. Heparin's mechanism is downstream at the common pathway, not at the level of factor activation via tissue factor or contact activation.
Point 4 represents fibrin clot formation. Direct thrombin inhibitors such as argatroban act closer to this point. Heparin acts upstream by inhibiting thrombin before it can convert fibrinogen to fibrin.
Pain unrelieved by opioids, tense shiny skin, and pain with passive stretch are hallmark signs of early compartment syndrome. Intact pulses are misleading, absent pulses indicate late irreversible ischemia, meaning this presentation is still an emergency. Fasciotomy is required and this exceeds LPN scope. Immediate escalation to the RN is the only appropriate action.
Administering a PRN opioid delays escalation and masks a worsening emergency. Pain unrelieved by opioids is itself a red flag, adding analgesia does not address the cause.
Elevating the limb is contraindicated, it reduces arterial perfusion pressure, worsening ischemia. Elevation is appropriate for edema but actively harmful in compartment syndrome.
Applying ice causes vasoconstriction, further reducing perfusion to already-compromised tissue, accelerating ischemic damage.
Pain unrelieved by opioids, tense shiny skin, and pain with passive stretch are hallmark signs of early compartment syndrome. Intact pulses are misleading, absent pulses indicate late irreversible ischemia, meaning this presentation is still an emergency. Fasciotomy is required and this exceeds LPN scope. Immediate escalation to the RN is the only appropriate action.
Administering a PRN opioid delays escalation and masks a worsening emergency. Pain unrelieved by opioids is itself a red flag, adding analgesia does not address the cause.
Elevating the limb is contraindicated, it reduces arterial perfusion pressure, worsening ischemia. Elevation is appropriate for edema but actively harmful in compartment syndrome.
Applying ice causes vasoconstriction, further reducing perfusion to already-compromised tissue, accelerating ischemic damage.
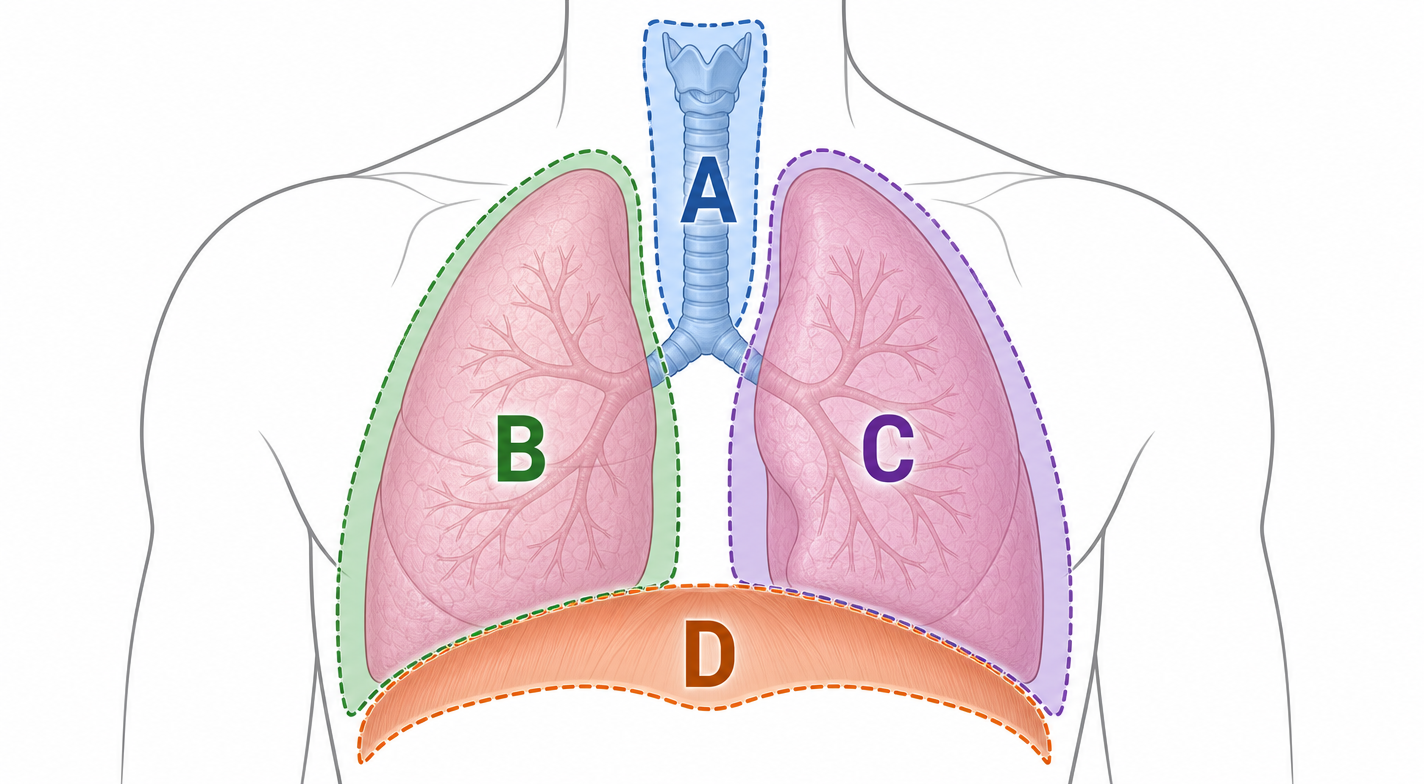
Absent breath sounds on the left with tracheal deviation to the right describe tension pneumothorax in the left lung, Zone C on this diagram. The diagram shows the patient facing the viewer, so the patient's left lung appears on the right side of the image. Air accumulation in the left pleural space compresses the lung and shifts mediastinal structures rightward. This is a life-threatening emergency. The LPN must escalate to the RN immediately; needle decompression is not within LPN scope.
Zone A is the trachea. Rightward deviation is observed here as a consequence of pressure buildup in Zone C, it is the effect, not the site of primary pathology.
Zone B is the right lung. Breath sounds are present on the right, this is the unaffected side. Tracheal deviation toward the right confirms the problem originates contralaterally in Zone C.
Zone D is the diaphragm. Diaphragmatic pathology would not produce unilateral absent breath sounds with tracheal deviation, this zone is not involved in this presentation.
Absent breath sounds on the left with tracheal deviation to the right describe tension pneumothorax in the left lung, Zone C on this diagram. The diagram shows the patient facing the viewer, so the patient's left lung appears on the right side of the image. Air accumulation in the left pleural space compresses the lung and shifts mediastinal structures rightward. This is a life-threatening emergency. The LPN must escalate to the RN immediately; needle decompression is not within LPN scope.
Zone A is the trachea. Rightward deviation is observed here as a consequence of pressure buildup in Zone C, it is the effect, not the site of primary pathology.
Zone B is the right lung. Breath sounds are present on the right, this is the unaffected side. Tracheal deviation toward the right confirms the problem originates contralaterally in Zone C.
Zone D is the diaphragm. Diaphragmatic pathology would not produce unilateral absent breath sounds with tracheal deviation, this zone is not involved in this presentation.
Dark urine, flank pain, fever, chills, and hypotension during transfusion describe acute hemolytic transfusion reaction, caused by ABO incompatibility. Free hemoglobin from lysed RBCs precipitates in renal tubules → acute kidney injury, especially dangerous with existing CKD. Stopping the transfusion immediately while maintaining IV access is the priority. This exceeds LPN independent management, immediate RN notification is mandatory.
Slowing the transfusion is appropriate for febrile non-hemolytic reactions, which present with mild fever without hemodynamic compromise. Hypotension and dark urine indicate hemolytic reaction, slowing does not stop ongoing hemolysis and delays critical intervention.
Antipyretics address fever symptomatically but do not stop the underlying hemolysis. Administering antipyretics without stopping the transfusion allows continued exposure to incompatible blood, worsening the reaction.
Obtaining a urine sample is part of post-reaction protocol but is not the immediate priority. Continuing to monitor while the transfusion runs allows ongoing hemolysis, assessment follows cessation, not the reverse.
Dark urine, flank pain, fever, chills, and hypotension during transfusion describe acute hemolytic transfusion reaction, caused by ABO incompatibility. Free hemoglobin from lysed RBCs precipitates in renal tubules → acute kidney injury, especially dangerous with existing CKD. Stopping the transfusion immediately while maintaining IV access is the priority. This exceeds LPN independent management, immediate RN notification is mandatory.
Slowing the transfusion is appropriate for febrile non-hemolytic reactions, which present with mild fever without hemodynamic compromise. Hypotension and dark urine indicate hemolytic reaction, slowing does not stop ongoing hemolysis and delays critical intervention.
Antipyretics address fever symptomatically but do not stop the underlying hemolysis. Administering antipyretics without stopping the transfusion allows continued exposure to incompatible blood, worsening the reaction.
Obtaining a urine sample is part of post-reaction protocol but is not the immediate priority. Continuing to monitor while the transfusion runs allows ongoing hemolysis, assessment follows cessation, not the reverse.
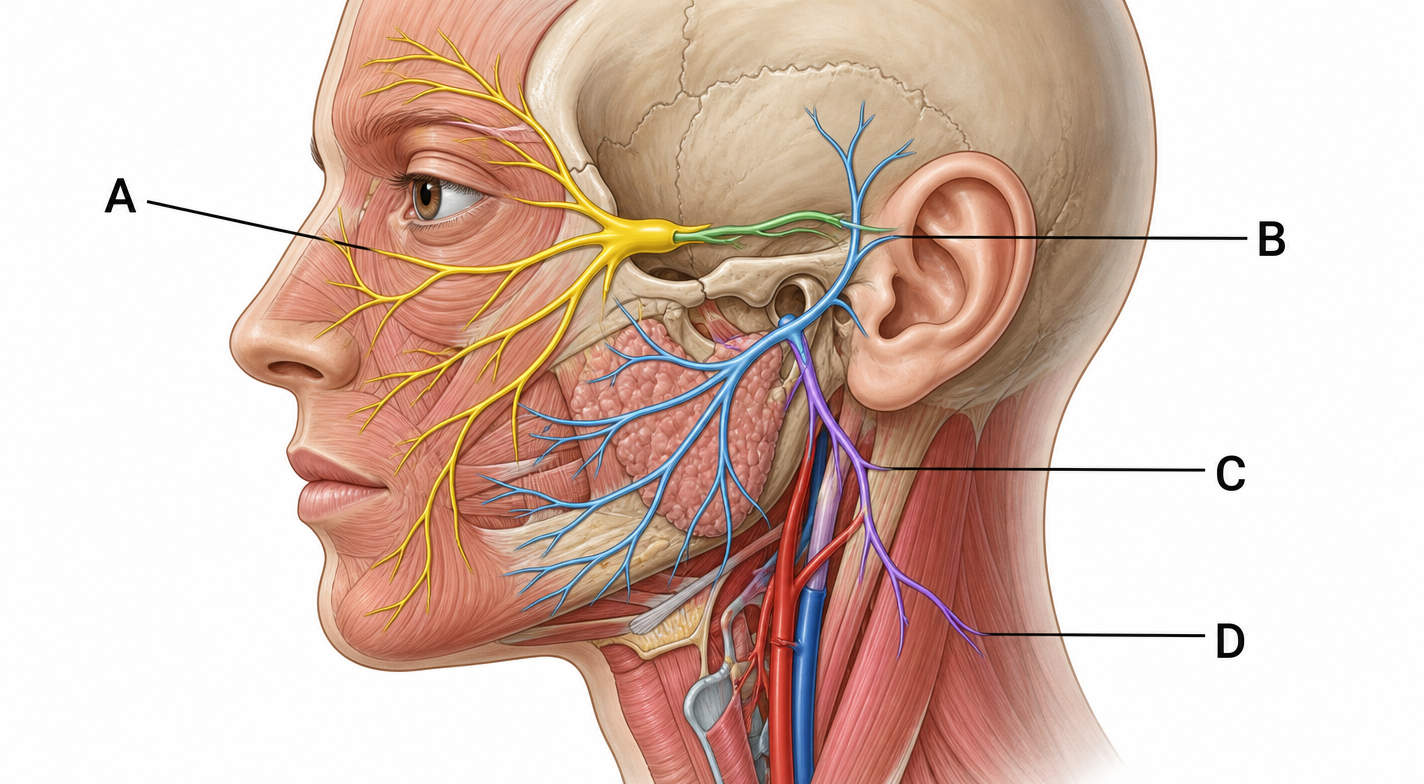
Inability to close the eye, facial drooping, and loss of taste on the anterior two-thirds of the tongue are classic signs of facial nerve (CN VII) palsy, Bell's palsy. Nerve A represents CN VII, branching through the parotid region across the face, controlling muscles of facial expression and carrying taste from the anterior tongue. The LPN should report findings, ensure eye protection with artificial tears and an eye patch to prevent corneal damage, and document progression.
Nerve B represents a branch near the auricular region. Lesions here would not produce the described combination of facial muscle paralysis and anterior tongue taste loss.
Nerve C represents cervical branches descending into the neck. This distribution does not innervate facial muscles or carry taste sensation, it cannot account for facial drooping or eye closure failure.
Nerve D represents deeper cervical structures. Pathology at this level affects neck musculature, not the superficial facial muscles or anterior tongue taste fibers implicated here.
Inability to close the eye, facial drooping, and loss of taste on the anterior two-thirds of the tongue are classic signs of facial nerve (CN VII) palsy, Bell's palsy. Nerve A represents CN VII, branching through the parotid region across the face, controlling muscles of facial expression and carrying taste from the anterior tongue. The LPN should report findings, ensure eye protection with artificial tears and an eye patch to prevent corneal damage, and document progression.
Nerve B represents a branch near the auricular region. Lesions here would not produce the described combination of facial muscle paralysis and anterior tongue taste loss.
Nerve C represents cervical branches descending into the neck. This distribution does not innervate facial muscles or carry taste sensation, it cannot account for facial drooping or eye closure failure.
Nerve D represents deeper cervical structures. Pathology at this level affects neck musculature, not the superficial facial muscles or anterior tongue taste fibers implicated here.

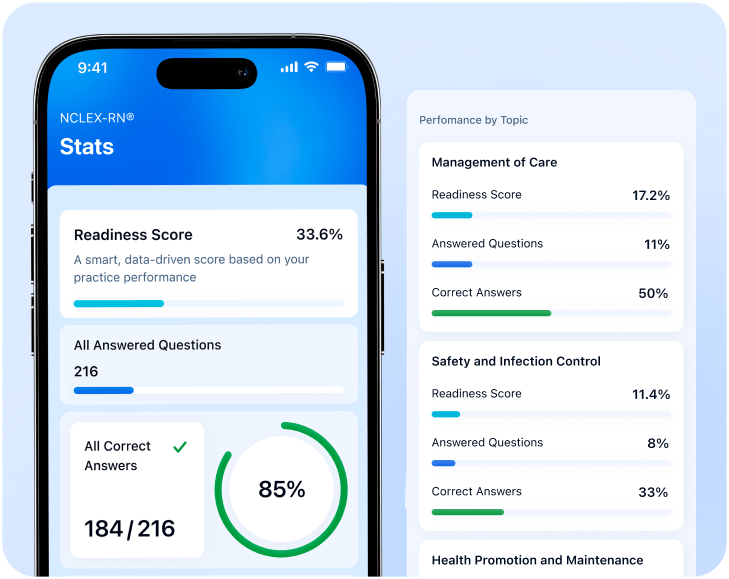
A personalized study plan is waiting!
Take a quick 3-minute quiz to prepare for NCLEX faster and more effectively.
Achieve 99% NCLEX® readiness with a clear strategy and without stress

Select all that apply
Rate it from 1 to 5
Reduce your stress with:

Stay confident with:

Rate it from 1 to 5
Select all that apply
See what students say about ExamReady:

 Verified
Verified
I work long shifts so studying for hours wasn't realistic. This app helped me use short breaks during the day. The quick quizzes made studying feel doable.
Verified
I was jumping between YouTube, textbooks, random sites and it was chaos. Here the quizzes and cheat sheets cover all the topics. I finally stopped feeling lost.
Verified
Some topics just wouldn't stick for me no matter what I tried. What helped most was reviewing missed questions. Going back to my weak areas really built my confidence.
Select all that apply
Quizzes with expert explanations and high-yield cheat sheets improve understanding and retention.
Select all that apply — your choices won't limit your experience
Plus, you get unlimited practice, progress tracking, and full 24/7 access

Small daily steps lead to big results
Create a study routine that fits your life



Achieve 99% NCLEX® readiness with a clear strategy and without stress
Rate from 1 to 5
Expert-built quizzes, clear explanations, and powerful tools — all to make prep easier and more effective
Rate from 1 to 5
Rate from 1 to 5
Rate from 1 to 5
Rate from 1 to 5
Passing the NCLEX on the first try can be challenging — we know how to help you focus, study your way, and see real results
*92% of ExamReady students report better focus and consistency after just one week
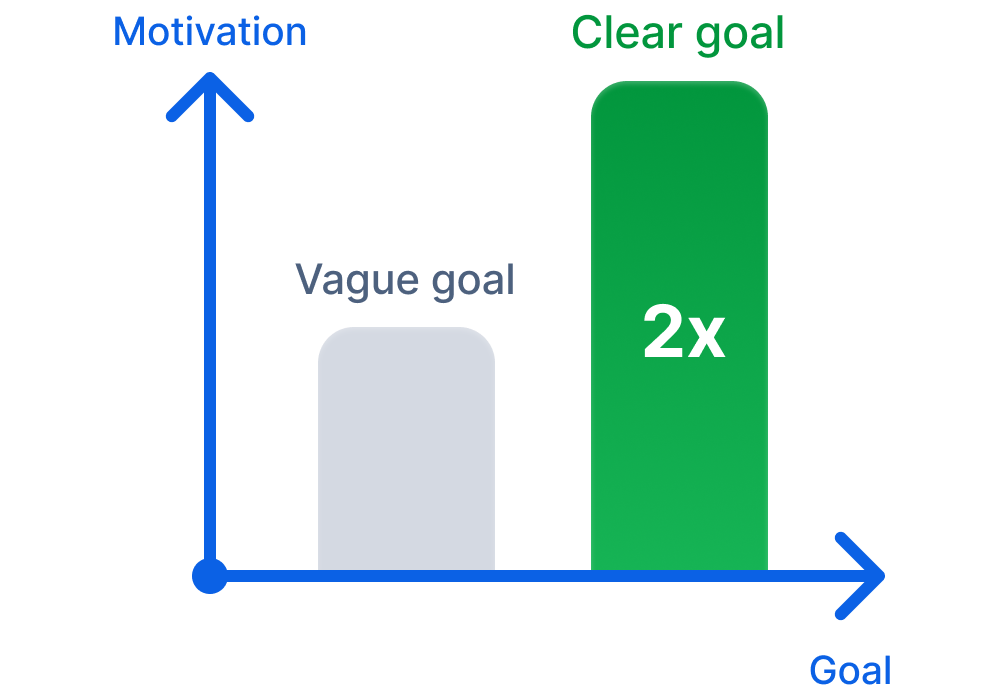
When you know exactly why you're studying, it's easier to stay focused — even when it gets tough
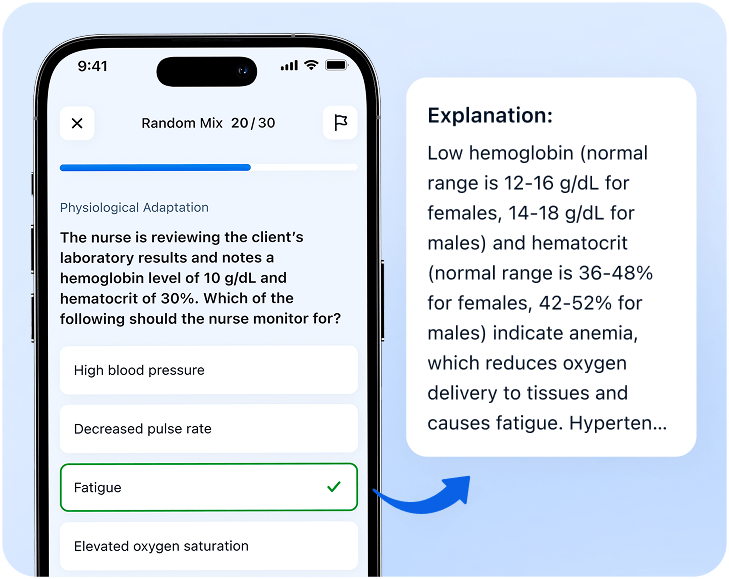
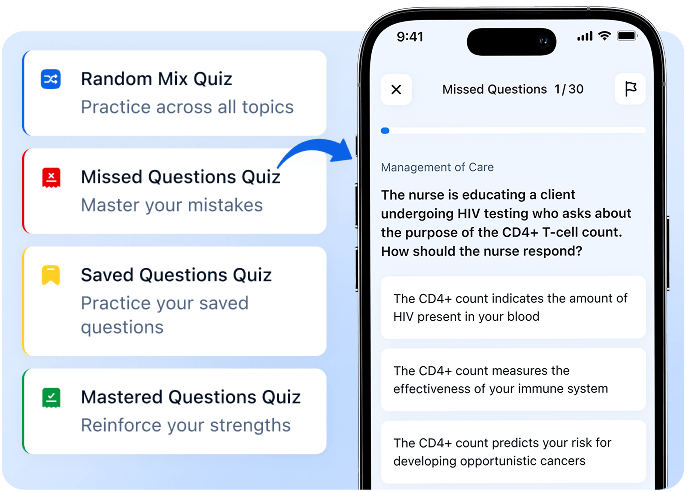
Master every topic with practice questions & clear explanations
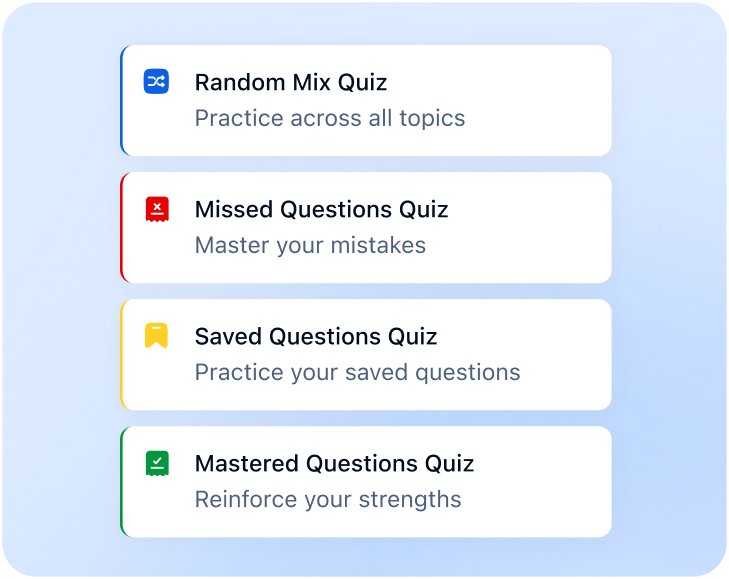
Save time and prepare efficiently with smart quiz modes
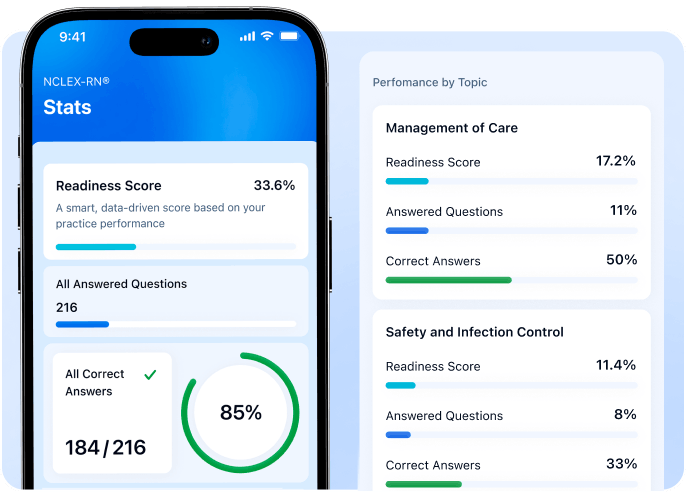
Track your progress, strengthen weak areas, and stay exam-ready
Select all that apply — your choices won't limit your experience
Rate from 1 to 5

Small daily steps lead to big results
Create a study routine that fits your life
Expert-reviewed content
Nurse Practitioner, 16+ years clinical experience
Certified Nurse Educator, NCLEX® Specialist
NCLEX® Prep Instructor, Former Clinical Nurse
and a broader clinical faculty team ensuring accuracy and quality
Verified
I had limited time to prepare for my exam, but this app made it easy. Clear explanations and a smart plan helped me pass on the first try!
Verified
I was so stressed about NCLEX until I found this app. It broke everything into manageable parts and helped me stay motivated. I felt calm on test day, and it paid off.
Verified
The quiz modes were a lifesaver! 'Missed Questions' helped me fix weak spots, and 'Saved Questions' let me review before my exam. Super effective and easy to use!

Your plan includes a gift: NCLEX® Cheat Sheets

Based on your answers, we've created a plan for 99% NCLEX® readiness
Recommended
by practicing nurses
We want you to start your journey with a nice surprise
Applied automatically at checkout
 NCLEX_26
NCLEX_26
To move forward, specify